
Stretch Training (Physiology)

Introduction
Flexibility is one of the key physiological factors involved in nearly all forms of human movement. It is also an essential component of general health, fitness, and sport-specific conditioning. Flexibility exercises have often been advocated by fitness professionals and sports coaches as a means of inhibiting and treating injuries and a way to develop sporting performance. Interestingly, we all have some indication of what flexibility is, yet there is no acceptable definition of it in the scientific literature. This has, unfortunately, lead to misinterpretations of the term flexibility, misapplications of the theory, and resulting difficulties not only in researching this physiological parameter but also in the application of evidence generated from such research.
It is important, to begin with, a well-defined understanding of what flexibility really is. To attain this, it is important to critically evaluate previous attempts to define flexibility, formulate a new and improved definition of the term, draw a distinction between the two main components of flexibility, and discuss the different ways of demonstrating and measuring this parameter.
One-Word Definitions
One-word definitions are unfortunately problematic and are often common. Flexibility has been defined informally as mobility, compliance, and alternatively as the reciprocal counterpart of stiffness. (Shier, 2000). The difficulties with such accounts are clear enough. First, the assumed synonyms are hardly equivalent. It can be specified that structures can be mobile without being flexible. "Compliance" equally implies yielding to a broad range of external demands, although the human body conforms to many such demands where flexibility is not necessitated. For example, the human body tolerating gravitational and atmospheric pressure. Even if such terms were identical, issues would still ensue because the definitions would be vague, repeating what the term means rather than providing an analysis. Likewise, the reciprocal counterpart of flexibility may definitely be stiffness, an examination of the meaning of "flexibility" is inadequate.
Range-of-Motion Definitions
Generally, researchers have defined flexibility as either the range of motion or as the range of motion at or approximately near a joint (Holt, Pelham, and Holt, 2008). The latter is favoured since the term range of motion is too general. A substantial issue with these broad definitions is that they obscure the actual property in question (flexibility) with the criterion we use to assess it (range of motion) (Holt, Pelham, and Holt, 2008). A joint's flexibility determines and is displayed by its range of motion, but the two are not equal. While the range of motion may aid as an appropriate operational definition, this criterion is seldom acknowledged.
Ability Definitions
Some definitions consider the need to differentiate flexibility from the criterion of its measurement. According to ACSM (2000) flexibility is the ability of a joint to move throughout its range of motion. Evidently what ought to be detailed is the potential range of motion, because every joint is able to move throughout the range of motion it actually has, however extensive or restricted the range is.
However, it is worth considering that if flexibility is the ability to move throughout a joint's potential range of motion, then any joint whose actual range is restricted of its potential will not be classified as flexible at all. This is because it will lack, the requisite ability (Holt, Pelham, and Holt, 2008) as the potential range of motion is a variable factor among others in determining flexibility.
The main difficulty is the phrasing, as the term "ability" is somewhat ambiguous, it could be better phrased as flexibility is the ability of a joint that determines its range of motion. Unfortunately, the term ability is then brought into question (ability to do what). These inconsistent terms create overall problems that restrict in creating a clear definition of what flexibility is.
A New Definition by Holt, Pelham, and Holt (2008)
Holt, Pelham, and Holt (2008) recognised the various inadequacies of previous attempts identified above and offered the following definition, “Flexibility is the disposition of body tissues to allow, without injury, excursions at a joint or set of joints.” The authors characterised flexibility as a specific type of disposition of body tissues. Additionally, Dantas (8) defined flexibility as a ‘physical feature responsible for the voluntary execution of a maximum joint range of motion, by a single or multiple joints, within morphological limits, without a risk of injury’. Regardless of the terms used to endeavour to define flexibility, it is clear to say that there are profound benefits of improved joint flexibility.
According to the ACSM position stand (1998, 2000) flexibility is an essential component of physical aptitude that can promote several benefits including reduced risk of injuries and enhanced athletic performance (Neilson and Bandy, 2005). Thus good flexibility may result in significant benefits for both the general population and athletes.
Stretching promotes muscle relaxation, defined by Dantas (2011) as ‘suspension of muscle tension’. Therefore, it could be conjectured that if there is increased muscle tension can cause individuals blood pressure to be elevated with problems with muscle irrigation, leading to reduced oxygenation and nutrient supply (Rubini, Costa and Gomes, 2007). Rubini and colleagues reported that this muscle tension could inhibit the removal of elements ensuing from muscle action, which escalates the amount of toxic residue accumulated in cells and predisposes muscles to pain and fatigue.
It is important to recognise that a muscle that is contracted expends energy needlessly. Therefore, if a muscle is constantly contracted, it becomes reduced in length, less flexible and more susceptible to injuries caused by unexpected movements requiring a greater range of motion (Alter and Alter, 2004). Muscle contraction can be either voluntary or involuntary and are largely neural, not muscular origin, initiated when a muscle is in a shortened position and contracts further. For example, muscular cramps typically dissipate when the affected muscle is passively stretched or when its antagonist is contracted. This technique is applied in proprioceptive neuromuscular facilitation (PNF) methods, due to stimulation of the Golgi tendon organ (GTO) (Guissard and Duchateau, 2006).
Flexibility is applicable throughout the ageing process, provided the physiological changes at given stages are considered (particularly in children and the geriatric populations) (Dantas et al. 2002). This consideration is due to the development in the longitudinal growth phase in children as their bones and soft tissues do not grow at the same rate. Bones may grow more rapidly than muscles and their connective tissues, thereby increasing muscle tension. At certain stages of development, the connective tissue may exceed bone growth, producing hyper-mobility and leaving the joint susceptible to sprains.
The consideration towards flexibility in early school-age children has been reported by Weineck (2004) who stated that ‘contradictory tendencies can be identified during mobility development in this age group. On one hand, the flexion capacity of the hip and shoulder joint, as well as the spine shows the highest mobility at 8-9 years of age. On the other, a decrease is observed in capacity to extend the legs apart at the hip joint and dorsally directed mobility in the shoulder joint.’ (Weineck, 2004 p.277). Further, Weineck specified that both muscles and ligaments do not develop at a paralleled rate with bone growth at the onset of adolescence because of accelerated growth and reduced tensile mechanical strength in the passive locomotor apparatus. Weineck further suggested that ‘care must be taken to ensure a balanced relationship between load and the capacity to support them, avoiding exercises performed with partners, unilateral and twisting movements, as well as torso hyper-flexion and hyperextension’ (Weineck, 2004 p.277).
Farinatti et al. (1998) investigated a study on 901 boys and girls (n = 487 boys; n = 414 girls) aged between five-to-15 years assessing joint mobility (flexitest). The results revealed that younger children exhibited greater flexibility than older children. This increased joint mobility was due to greater articular mobility since the younger children’s ligaments and joints were not fully developed. In older children, there was an increase in tensile strength and a gradual reduction in articular mobility.
As specified earlier, during the latter stages of the ageing process in adults the range of motion at the joint decreases due to developed connective tissue and a reduction in muscle fibre elasticity. Older adults degenerative processes including impaired mobility may contribute to a lower range of motion and pathologies correlated to the musculoskeletal system. Functional decline ensues that leads to various losses in sensory and motor control. Weineck (2004) stated that during the ageing process ‘alterations in active and passive locomotor apparatuses, cardiovascular and cardiopulmonary systems are mainly responsible for decreased physical performance capacity.’ Unfortunately, many of these conditions are permanent, although physical activity may partly re-establish the functional skills and psychological capacity of the elderly adult. Applying stretching adequate for the older adult population might contribute to diminishing the ageing effects, provided the exercises are appropriately and safely adjusted to meet the needs of each individually.
The Mechanisms Affecting Flexibility
Unfortunately, studying flexibility is an exceedingly complex subject and therefore creates significant challenges when investigating it. The main challenges are generally due to the variety of intervening mechanisms. There are four elements that are predominantly responsible for the degree of joint flexibility: (1) mobility; (2) elasticity, (3) plasticity; and (4) pliability (Dantas, 2005). Joint mobility is the amount (degree) of joint movement and accounts for 47% of flexibility resistance. Elasticity refers to the stretching of muscle components, contributing to 41% of flexibility resistance. Plasticity refers to the level of plastic component deformation during flexibility exercises, its residual post-exercise deformation being termed hysteresis. Pliability refers to skin changes in the section required for the movement.
Proprioception Mechanisms
The musculoskeletal system (locomotor apparatus) is not the only factor affecting flexibility. The nervous system regulates (in part) the range of motion, muscle tension, and restricts the range of joint motion thus reducing injury potential. Proprioception in this system may be associated with joints or muscles (Hong, Molland and Sullivan, 2010).
Joint proprioceptors are formed by Pacinian and Ruffini corpuscles. Their function is to provide joint location sense, the velocity of movement and information on the resistance that resists the movement. There are several different types of sensory receptors located in the joint capsules and ligaments (Guissard and Duchateau, 2006). Muscle proprioceptors are formed by the muscle spindle and the Golgi tendon organ (GTO). The muscle spindle is located in muscle fibre (Figure 2). When a muscle is stretched, the central portion of the muscle spindle called the nuclear bag accompanies the movement and is ‘pulled back’, activating the sensory terminals called annulospiral endings (Figure 2). These transmit impulses to the medulla, where synapses are made with α-motoneurons. After stimulation, they transmit information to contract extrafusal fibres (myotatic reflex) (Hsich et al. 2009).
The GTO is situated near the insertion point of muscle fibre in the tendon. Typically they are 10-to-15 muscle fibres that are attached directly to each GTO, which responds to the tension produced by the bundle of muscle fibres. Nerve impulses discharged by the GTO are transmitted by fast conducting afferent axons to the spinal medulla and cerebellum. Upon reaching the medulla, those impulses excite inhibitory interneurons that discharge an inhibitory neuromediator (γ-aminobutyric acid [GABA]). This acts on α-motoneurons, inciting muscle relaxation.


Figure 1. Receptors in the motor system. Golgi tendon organs (GTOs) and muscle spindles are two types of specialised receptors associated with skeletal muscle. Extrafusal muscle fibres comprise most of the muscle and are innervated by alpha motor neurons. The GTOs are positioned at the junction between extrafusal muscle fibres and the tendon (in series) and are innervated by only one afferent fibre, the type Ib afferent. Located within the fleshy part of skeletal muscle (in parallel) are the muscle spindles. The spindles are composed of intrafusal fibres innervated by both afferent (types Ia and II) and efferent (gamma motor neuron) fibres. B, Each muscle spindle is composed of three types of intrafusal muscle fibres. The average muscle spindle contains one dynamic nuclear bag fibre, one static nuclear bag fibre, and three or more nuclear chain fibres. A group Ia (dynamic) fiber innervates every intrafusal fibre regardless of the number. A group II (static) afferent fibre innervates the static nuclear bag fibre and all nuclear chain fibres. Each intrafusal fibre also receives motor innervation to the distal (contractile) regions to control its overall length and sensitivity. The dynamic nuclear bag fibre is innervated by dynamic gamma motor axons, whereas the static nuclear bag fibre and all of the nuclear chain fibers are innervated by static gamma motor axons.
(Modified from Gordon and Ghez [1991]. Muscle receptors and spinal reflexes: the stretch reflex. In ER Kandel, JH Schwartz ; TM Jessell [Eds.]. Principles of neural science [3rd ed.]. New York)
Mechanisms of Flexibility
Flexibility performance is conditional directly on the different structures. Joints are formed by one or more bones, and movable (i.e. synovial) joints are the most essential for flexibility. Ligaments are another important structure that effects flexibility. Ligaments are strong fibrous cords of connective tissue, flexible but inelastic, which attach two bones (i.e. femur and the tibia). Their main purpose is to support a joint. Ligaments are comprised of bundles of collagen fibres are intertwined around each other; they are pliable and flexible, creating freedom of movement, but are resilient enough not to yield to the applied forces. Alter (2004) specifies that the joint capsule and ligaments account for 47% of the total resistance to movement.
Tendons are formed by fibrous tissue responsible for attaching a muscle to bone. They are essentially inextensible, offering around 10% of the total resistance to movement (Alter, 2004). The key function of tendons is to transfer muscle tension to the bones, thus creating movement. This structure is composed primarily of compressed parallel collagen fascicles of varying lengths and widths (Alter, 2004).
Muscles are a vital component of flexibility due to their elastic properties. Muscles are active organs composed of fibre bundles that allow for the production of voluntary and involuntary movements due to their contracting capacity. Therefore, muscles are the principal structure in flexibility performance. Muscle fibres are enclosed by the sarcolemma (cell membrane), covered by the endomysium (connective tissue) (Figure 3). The sarcolemma contains contractile proteins, enzymes, nutrition substrates, nuclei, organelles and the sarcoplasmic reticulum, where the muscle contraction process initiates (Silva et al. 2003). Muscle fibre groups form bundles (fascicles) surrounded by the perimysium. A set of fascicles is covered by epimysium (a sheath), forming a muscle. Fibres at muscle endings become increasingly infrequent and the connective tissue layers that enclose the muscles begin to compress, forming tendons, which insert directly into the bones. The functional unit of a muscle is the sarcomere, composed of myofilaments of actin (thin) and myosin (thick), bordered by the Z-line. Each sarcomere includes almost 450 thick filaments at the centre and 900 thin filaments at the ends. Several sarcomeres form the myofibril, filaments that slide over each other producing muscle contractions (Allen, Zhang and Whitehead, 2010).
The actin and myosin filaments are inextensible and only contribute to muscle contractions, without altering their length during sarcomere extension. However, a third filament (titin) takes part in the extension of a smaller functional muscle unit (Trinick and Tskhovrebova, 1999). The thick filament (myosin) is attached to both ends of the Z-line via titin, accountable for increased sarcomere length. The length of this filament is what regulates the amount of sarcomere stretching. According to Trinick and Tskhovrebora, the titin molecule resembles a chain and consists mainly of immunoglobulin and fibronectin. It forms a link between the Z-line and A-band and is the third type of sarcomeric filament. Titin is responsible for muscle composition and elasticity, thus being an essential element in muscle stretching due to unfolding inside the sarcomeres, the smaller functional units of a muscle (Silva et al. 2003).
From a mechanical standpoint, the locomotor apparatus can be separated into elastic, plastic and inextensible components. During muscle stretching, both the elastic and plastic muscle mechanisms are deformed. The elastic components formed by connective tissue and myofilaments return to their original state after muscle relaxation. The connective tissue due to its disposition incites involvement of the parallel elastic components surrounding both the sarcolemma/endomysium and the perimysium, and series elastic components (Fung, 1993). Plastic components, composed of mitochondria, reticulum, the tubular system, ligaments and intervertebral discs, do not return to their original state after stretching. Inextensible components are made up of bones and tendons. Tendons are not affected by training; ligaments, however, adjust to stretching, since they do not return to their original state. Therefore, a ligament that is continually injured may become loose and inhibit its functional role.

Figure 2. A schematic representation of a skeletal muscle in cross-section showing the organisational structure of the muscle bundles (fasciculi) and fibres with their respective surrounding layers of connective tissue.
Diagram by Marley Dobyns, Animal Science Department, Iowa State University.
Acute Effects of Stretching
When a muscle or muscle group is passively stretched using static, dynamic, or proprioceptive-neuromuscular facilitation (PNF) stretching may produce some acute alterations in the muscle. Acute effects of stretching on muscle relate to the early performance alterations in the first few hours after performing stretching. The acute effect ensuing after performing stretching, therefore, depends on the biomechanical performance variable of interest. Some biomechanical variables (i.e. range of motion) have been reported to improve stretching, while others have been unaffected (stiffness) or significantly diminished (strength).
An essential aspect in the acute effect of stretching is that of passive tension in a muscle which is dependent on the rate of the applied stretch. This rate dependency means that the tensile resistance in a muscle depends on the scheduling of the stretch (viscoelasticity). The faster the stretch the greater the stiffness of the muscle will be. Stiffness is the degree of elasticity of a material and is defined as the slope of the load/deformation curve in the elastic region of the curve. The load-deformation curves of viscoelastic materials are complex and have several regions. If these tissues were pulled to failure the curve would show a “plastic” region where the curve flattens out as lasting damage is produced to the tissue.
During normal daily activities, most ligament and tendon strain is typically between two to five per cent strain (Carlstedt and Nordin, 1989). The viscoelastic response of muscles, tendons, and ligaments means that a slow stretch will create less passive tension than a faster stretch to the same length. Kubo et al. (2002b) investigated the acute effects of stretching and contractions on the stiffness of the human Achilles tendon. The acute effect of stretching significantly decreased tendon stiffness (8%), but the largest effect of stretching was a 29% reduction in hysteresis. Hysteresis is the energy lost when a viscoelastic material is stretched and returns to its normal length.
Stretching Practices and Exercise Prescription
Flexibility is comparable to aerobic capacity, strength, hypertrophy and neuromuscular endurance in being a modifiable fitness element. Research into appropriate exercise prescriptions for slow/static, dynamic stretching is still limited. Even fundamental recommendations for safe and effective use of these stretching techniques are incomplete. This section provides some practical procedures for the use of static, dynamic stretching techniques and proprioceptive neuromuscular facilitation (PNF).
There are several types of flexibility: (1) static; (2) dynamic; (3) ballistic; (4) and controlled (Figure 3). Static flexibility is the most common method performed and occurs when the individual maintains a position, moving the body segment slowly and gradually until the maximum articular arc has been extended. This mode of flexibility is most commonly used to evaluate pre-to-post levels of flexibility. It is characterised by the maximum range of motion achieved during the performed movement and is used significantly in the sport and fitness industry. A number type of movement performed is ballistic flexibility which forces the limb into an extended range of motion when the muscle is not relaxed enough to enter it. It involves fast repeated bouncing movements and is widely used by ballerinas, athletes and gymnasts.

Slow/Static Stretching
The traditional belief that stretching is advantageous has circulated and practiced for thousand of years, especially in preparing for combat (Behm, 2018). However, the preferred mode of stretching during the early years was static stretching. This general belief that static stretching produced increased flexibility and augmented athletic performance gathered momentum from the World Wars until the early 1990’s (Behm, 2018). This was developed from the credence that by increasing individuals range of motion reduces resistance to movement thus improving their economy of movement.
Most static stretching practices involve individuals performing a succession of three-to-five repetitions, each lasting 10-to-20 seconds. Interesting, this is even though research has reported less than 30 seconds to be ineffective. The performance of the slow/static technique involves a controlled constant movement to the end range. This can be via gravity or other external force, a concentric contraction of the antagonists, or a combination of the two (slow phase). At the end range, the Individual holds the terminal position for the selected time. After the static hold phase, the individual returns to the starting position and then repeats the movement. The quadriceps stretch is an example of a slow/static stretch protocol (Figure 4).
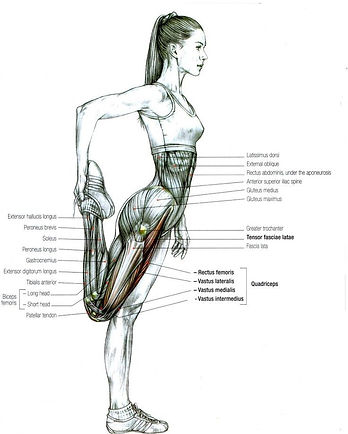
Figure 4. The standard quadriceps stretch.
Slow/static stretching traditionally has been used as part of a warm-up before exercise or sport (ACSM, 2000). It was generally believed that pre-exercise static stretching would promote better performance and reduce the risk of injury (Shellock and Prentice, 1985; Smith, 1994). These recommendations stated that all the major muscle groups could be stretched, and was a simple and generally safe method. However, reassessment on the effect the pre-exercise static stretching has on strength, power and explosive muscular performance has thrown doubt on this belief.
Recent reviews have suggested that pre-exercise static stretching may essentially decrease performance (Shrier, 2004; Rubini et al. 2007; McHugh and Cosgrave, 2010; Behm and Chaouachi, 2011). More importantly, contemporary reviews have reported that stretch-induced reductions in performance are apparent in maximal and explosive muscular efforts that play an essential role in a number of individual and team sports (Markovic and Mikulic, 2010; Cormie et al. 2011). These results have already made an impact on sports and exercise professionals who now start to recommend avoidance of static stretching during warm-up for sport and exercise (Pearson, 2001; Young and Behm, 2002; Knudson, 2007).
Evidence on Strength and Power
Simic and colleagues (2012) performed a meta-analysis of the acute effects static stretching had on muscle strength, power, and explosive muscular performance. A total of 104 studies met the inclusion criteria and yielded 61 data points for strength, 12 data points for power and 57 data points for explosive power. The pooled estimates for maximal muscle strength (peak force, torque, or 1RM) reported that static stretching had an acute negative acute (-5.4% [95% CI: -6.6% to -4.2). Subgroup analyses displayed comparable acute effects of static stretching on maximal muscle strength in both athletes and non-athletes (P = 0.97). Furthermore, subgroup analysis reported that pooled estimates for the acute effect of static stretching on isometric and dynamic strength tests were -6.5% (95% CI: -8.3% to -4.6%;) and -3.9% (95% CI: -4.8% to -2.9%) respectively.
The pooled estimate of the acute effect of static stretching has on muscle power reported -1.9% (95% CI: -4.0% to 0.2%), indicating an unclear acute effect of static stretching on muscle power. Subgroup analyses displayed comparable acute effects of static stretching on muscle power in both athletes and non-athletes (P = 0.7). For all explosive muscular performance tests, the pooled estimate of the acute effect of static stretching was -2.0% (95% CI: -2.8% to -1.3%), indicating a negative acute effect of static stretching on explosive muscular performance. Subgroup analyses showed a similar acute effect of static stretching on explosive muscular performance in both athletes and non-athletes (P = 0.81).
Simic and colleagues (2012) concluded that static stretching prior to exercise has negative acute effects on maximal muscle strength and explosive muscular performance, while the corresponding acute effects on muscle power remain uncertain. Based on the evidence from this study, caution should be taken with the usage of static stretching as the sole activity during warm-up practices and should largely be avoided.
Recently, Chaabene et al. (2019) have attempted to summarise previous and current findings on the acute effects of static stretching on sporting performances (Table 1). The Chaabene and colleagues have recommended that short-duration (<60 seconds) static stretching should be integrated within a warm-up component prior to the participating in recreational sports activities due to its potential positive effect on flexibility and musculotendinous injury prevention. However, in high-performance athletes, short-duration static stretching has to be applied with caution due to its negligible but still prevailing negative effects on ensuing strength and power performances, which may have an impact on performance during competition. It is however, clear that further investigations are required and also updating of established recommendations.
Figure 4. Various types of stretching.
Table 1. Progression of Scientific Evidence Through Time on Static Stretching (Adapted from Chaabene et al. (2019])
Essential Reading & Resources (Click Image For External Source)









Dynamic Stretching
A well performed sport action often includes the storage and release of elastic energy together with the accurate control of muscle contractions. When co-ordinated correctly, this can result in the fast limb movements required for success in the vast majority of sports. As mentioned in table 2, dynamic stretching in the late 1990’s-to-early 2000s has been promoted as a superior sport-specific technique.
Dynamic stretching generally involves trainees completing between five-to-15 repetitions. Some sports coaches consider dynamic stretching as a superior method of improving athletes dynamic flexibility, others, however, suggests that it exposes the athlete to a greater potential of unnecessary injury. However, research from 1990’s-to-early 2000s suggests that if it is performed progressively, under control, and without excessive resistance, dynamic stretching can be an important preparatory aid to sporting performance (watch the awesome video below from he NSCA’s 2018 Personal Trainers Conference).
YouTube Video on Dynamic Warm-Up for Speed & Power Athletes (Credit NSCA.com and Bobby Smith
Research From Late 1990’s-to-Early 2000s
Dynamic stretching has been defined as ‘the ability to use a range of joint movement in the performance of physical activity at normal or rapid speed’ (Alter, 1996). Alter suggests that this type of flexibility is more appropriate to sports specific exercise as it involves movement as opposed to static flexibility, which does not. Dynamic stretching has also been termed as ‘the ease of movement within the obtainable range of motion’ (Gleim & McHugh, 1997). Gleim and McHugh suggest that ‘stiffness’, which they describe as ‘the resistance of a structure to deformation’, is an important factor in dynamic stretching exercises that may impact injury risk.
As described earlier, muscles are viscoelastic in nature meaning that they are neither plastic nor elastic (muscle contains both collagen and elastin). Warming these muscles reduces viscosity, which has the effect of allowing the muscle to stretch more easily (Alter, 1996). This suggests that warming a muscle is important in decreasing the resistance to stretch. Many early studies support this belief and have reported that muscle tissue reduces in stiffness as the temperature of the muscle increases (Ekstrand, 1982; Franks, 1983; Safran, 1988; Noonan, 1993).
Another mechanism that is suggested to reduce the stiffness in muscle tissue is that of the production of glycosaminoglycans which are reported to be stimulated by stretching (Aro et al. 2008). These substances lubricate the tissue fibres inhibiting them from attaching, (Akeson et al. 1980). Wolpaw and Carp (1990) have also demonstrated that adaptive plasticity occurs in the central nervous system as a result of dynamic stretch training. This has the effect of increasing the point at which the stretch reflex initiates, which would allow the muscle to reach a greater length before a contraction in the same muscle would occur.
In the evaluation of pre-2010 dynamic stretching evidence, the scientific literature suggests that shorter durations of dynamic stretching do not negatively affect performance (Table 5), and longer duration of dynamic stretches may facilitate performances (Hough et al. 2009; Pearce et al. 2009; Yamaguchi et al. 2008). It is important to consider that several pre- 2010 dynamic stretch studies are inconsistent with limited descriptions provided concerning stretch intensity making it difficult to compare between studies. Although some studies do not report the dynamic stretch intensity (Manoel et al. 2008), others control the intensity by documenting the frequency of movement (Bacurau et al. 2009). Herman and Smith (2008) used a combination of dynamic activities and stretches and specified that they were performed at a slow to moderate tempo, but this was not accurately defined. A further difficulty is a definition of dynamic activities and dynamic stretches.
Table 5. Short term effects of dynamic stretching on performance (< 2010 studies)
Adapted from Behm & Chaouachi (2011).
There were various suggestions and potential mechanisms as to why dynamic stretching improved muscular performance. For example, Fletcher and Jones (2004) suggested this improvement was due to the elevated muscle and body temperature. However, others have suggested that improvements were because of a post-activation potentiation effect in the stretched muscle caused by voluntary contractions of the antagonist (Hough et al. 2009; Torres et al. 2008). Other studies (Jaggers et al. 2008; Yamaguchi and Ishii 2005) have reported that improvements were due to the stimulation of the nervous system, and decreased inhibition of antagonist muscles.
Houston and Grange (1990) hypothesised that dynamic stretching had a post-activation potentiation effect on performance via an increase rate of cross-bridge attachments. This was supported by Faigenbaum et al. (2005) and Yamaguchi and Ishii (2005) who suggested that the increases in force output after dynamic stretching are produced by heightened neuromuscular functioning. As a result of these and other studies findings, dynamic stretching was recommended as part of a pre-activity routine that may enhance force and power development (Hough et al. 2009; Torres et al. 2008; Yamaguchi and Ishii 2005).
Proprioceptive Neuromuscular Facilitation Stretching

In the late 1940s, Herman Kabat investigated as part of a rehabilitation program for patients with polio a stretching protocol known as proprioceptive neuromuscular facilitation (PNF). This approach was adopted by athletes in the late 1970s as a method of developing flexibility. PNF stretching is different from other forms of stretching as it incorporates a combination of different muscle actions (concentric, eccentric, isometric) and also passive stretching. The physiological rationale for this approach is to cause muscle relaxation via the inhibition of the agonist muscle group that would in facilitate greater ROM. Sharman and colleagues (2006) reported that by performing only one repetition of PNF stretching led to 3-to-9 dress acute response in subjects ROM. Research has suggested that several neural muscular mechanisms may play essential roles in muscle relaxation. One such mechanism is autogenic inhibition which involves the reflex relaxation that ensues in an agonist muscle group after fatiguing contractions via Golgi tendon organ stimulation. Furthermore, another mechanism called reciprocal inhibition involves antagonist muscle relaxation resulting from contracting the agonist muscle group.
Further evidence has suggested that isometric muscle action may marginally alter muscle spindle function to favour relaxation (Alter, 1996). It is also believed that PNF stretching increases athletes stretch tolerance or perception permitting a greater acute ROM and flexibility improvements (Sharman et al., 2006). Studies by Alter (1996) and (Sharman et al., 2006) have demonstrated that PNF stretching can increase flexibility by up to 33% and it is a superior mode of enhancing flexibility compared to static stretching. PNF stretching is believed to offer numerous benefits to athletes. The study by Caplan and colleagues (2009) reported that both PNF and static stretching alters stride length and in turn can alter sprint biomechanics by9.1% and 7.1% respectively. The work of Alter (1996) suggested that this may be due to the resistive component, with PNF stretching enhances muscle strength, endurance and joint stability. However, PNF stretching has been reported to have negative effects on strength and power activities when performed prior to the main exercise (Bradley et al., 2007). There are several variations of PNF stretching that individuals may perform. These variations involve the assistance of a partner or it can be self-applied. Four commonly used PNF methods include (i) hold-relax, (ii) contract-relax, (iii), hold-relax with agonist contraction, and finally (iv) contract-relax with agonist contraction. The term ‘hold’ makes reference to an isometric action and contract refers to the concentric contraction of the agonist or antagonist muscle group. Relax denotes to passive static stretching. To improve individuals flexibility it is suggested by Sharman et al., (2006) PNF stretching should be performed 1-to-2 days per week with a static contraction of at least 20% of the maximal voluntary contractile force. ACSM (2009) recommend a 6-second contraction followed by a 10-30second assisted stretch.
Excellent Youtube clip and explanation of Proprioceptive Neuromuscular Facilitation (PNF) Stretching Performed by Professor Mulvihill
Various PNF Methods
Hold-Relax
-
The technique begins with a passive stretch held at the point of mild discomfort for ∼10 seconds
-
Partner applies force to the antagonist's muscles and instructs athlete to hold the position
-
The athlete ISOM contracts and resists the partner’s force for ∼6 seconds
-
Athlete relaxes and partner passively stretches athlete deeper in the ROM for ∼20–30 seconds
-
The cycle may be repeated until the final segment of ROM is reached (Fig. 10.3)
Contract-Relax
-
The technique begins with a passive stretch held at the point of mild discomfort for ∼10 seconds
-
Partner applies force to the agonist muscle group while the athlete CON contracts the agonist group through the joint ROM
-
Athlete relaxes and partner applies passive stretch in the deeper area of ROM for ∼20–30 seconds
-
The cycle may be repeated until the final segment of ROM is reached
Hold-Relax with Agonist Contraction
-
Technique begins with a passive stretch held at the point of mild discomfort for ∼10 seconds
-
Partner applies force to antagonist muscle group and instructs athlete to hold the position
Essential Reading & Resources (Click Image For External Source)



References
-
Allen D., B. Zhang, N. Whitehead (2010) Stretch-induced membrane damage in muscle: comparison of wild-type and mdx mice. Muscle Biophys. 682:297-313.
-
Alter M. Alter M. (2004) Science of Flexibility (3rd ed.) Human Kinetics, Champaign IL.
-
Dantas E.H.M., S.A.M.Pereira, J.C.Aragão, A.H.Ota (2002) The preponderance of decreased joint mobility or muscular elasticity in the loss of flexibility in the aging process. Fitn.Perform.J. 1(3):12-19.
-
Dantas E.H.M., S.A.M.Pereira, J.C.Aragão, A.H.Ota (2002) The preponderance of decreased joint mobility or muscular elasticity in the loss of flexibility in the aging process. Fitn.Perform.J. 1(3):12-19.
-
Farinatti P., A.Nóbrega, C.Araújo (1998) Perfil da flexibilidade em crianças de 5 a 15 anos de idade. Revista de Educação Física e Desporto 14:23-31.
-
Fung Y.C. (1993) Biomechanics: Mechanical Properties of Living Tissues (2nd ed.) Springer-Verlag, New York.
-
Guissard N., J.Duchateau (2006) Neural aspects of muscle stretching. Exerc.Sport Sci.Rev. 34:154-158.
-
Hong J., M.Velez, A.Moland, J.Sullivan (2010) Acute effects of whole body vibration on shoulder muscular strength and joint position sense. J.Hum.Kinet. 25:17-25.
-
Nelson R., W. Bandy (2005) An update on flexibility. Strength Condit.J. 27:10-16.
-
Pollock M., G.Gaesser, J.Butcher, J.Despres, R.Dishman, B.Franklin, C.Garber (1998) ACSM Position Stand: The recommended quantity and quality of exercise for developing and maintaining cardiorespiratory and muscular fitness, and flexibility in healthy adults. Med.Sci.Sports Exerc. 30:975-991.
-
Rubini E., A.Costa, P.Gomes (2007) The effects of stretching on strength performance. Sports Med. 37:213-224.
-
Silva E., W.Z.Freitas, M.L.D.Ferrão, J.Fernandes Filho, E.H.M.Dantas (2003) Flexibility levels in terms of the muscular fiber type. Fitn.Perform.J. 2(3):157-164.
-
Trinick J., L.Tskhovrebova (1999) Titin: a molecular control freak. Trends Cell Biol. 9:377-380.